
Background on the use of video recording in primary care research
Primary care researchers began using video recordings to study consultations in the late 1970s.16 In one early study, a communication analyst videotaped primary care consultations with a single video camera and subsequently analysed the communication patterns between doctors and patients to improve doctors’ communication skills.17 The results showed that doctors’ communication styles affected patient satisfaction. Recent studies have used video data to analyse non-verbal communication cues to inform more effective doctor–patient interactions.18–20 Video data were also utilised to train doctors to improve their interactions with patients.16 In addition, studies have used video recordings to explore doctor–patient–computer interactions.21–29 These studies were instrumental in identifying the best spatial organisation of an exam room, better design of exam-room computers, impact of computer use on communication and effective use of the computer by the doctor during the clinical visit. Several studies also utilised video elicitation interviews (which are basically interviews done after the recording, asking the doctors or patients to reflect on what they see on the video) to analyse doctor–patient interaction in the visits for teaching purposes.30,31 Video elicitation allowed researchers to integrate the data from the video recording and participants’ related thoughts, beliefs and emotions obtained from the elicitation interviews.32 Although traditional observation can provide a range of interesting and insightful information about primary care encounters, the encounter occurs through complex and multiple interactions that can be explored by video data better. Finally, video data have also been used in health care settings in addition to primary care consultation for various purposes.33
Considerations for collecting Video Data in Primary Care
Video-recording methods require careful planning in order to gather data that effectively answer potential research questions. Table 1, which is derived from our experience of several studies,26–28 summarizes the steps to conduct a video observation study in a primary care setting for a given problem.
Some of the elements listed in different categories in Table 1 have inter-dependent nature, for instance, number of participants, time frame of the study, time needed for ethical approval and the instruments may all have mutual effect. Furthermore, video data might have ‘identifiable private information’ and involve human subject data, therefore require some additional requirements for IRB review.34 In video data collection, compared with traditional observation, studies conducted in US showed that physicians might have concerns about potential liability.35 Therefore, there should be a consensus between administrators and investigators about the purpose of the research and the methods used. Studies in US reported that it can also be effective to have some strategies to overcome doctors’ concerns with confidentiality and liability, such as obtaining certificates of confidentiality36 or becoming familiar with the liability coverage at the clinic where data will be collected.37 As added protection, a previous study reported that patients were generally less worried than doctors about being videotaped.32 However, it is still essential to get certificates of confidentiality to protect the participants’ identifiable information from forced disclosure. IRB approval requires confidentiality, but in the case of some sort of legal case (such as a malpractice case), the court might be able to force researchers to reveal this information. Certificates of confidentiality – which allow the investigator and others who have access to research records to refuse to disclose identifying information on research participants in any civil, criminal, administrative, legislative or other proceeding, whether at the federal, state or local level – might prevent this potential conflict between IRB and legal jurisdictions with respect to discoverability.38
Table 1 Steps followed to conduct this video study

With technological advancements, some researchers have started to use more complex video methods for data collection to capture all interactions in detail – such as body language and gazing direction.9,14,39 A multi-channel video might be a superior method to single-channel video depending on research question as it collects a greater amount of information, allowing the research to see both the care-provider and the patient simultaneously from different angles.14 For instance, some researches created a multi-channel video technique and software to capture all the computer use (including screen-capture, key stroke and mouse movement), and doctor–patient interaction in detail, which enabled them to view simultaneously all data relating to any time or activity.25 Another study used multi-channel video recording focussing on the patient’s face, the physician’s face and the overall interaction to capture eye gaze patterns.27,28
Furthermore, as video recording technology becomes more complex, researchers are faced with a wide variety of options, so it is important to choose the methods and equipment best suited to a given study. Researchers should standardise the camera operation protocols and have back up cameras in case of malfunctioning. In addition, multi-channel video and audio recording can collect so much data that the process of analysis becomes more complicated and time consuming. Therefore, it is essential to determine the specific research problems to minimise data collection and analysis time.
The Benefits & Drawbacks of Video Methods
Table 2 shows the pros and cons of traditional human observation method and video recording by ‘unmanned’ cameras. This table was established based on our own experience and previous studies.6,7,36,37,39,40–42
Video methods can be effective for research that can be conducted in a single room (for example, the patient exam room in a primary care clinic), since the cameras can be set up in a fixed position, specifically focussing on the interaction in the exam room. In addition, cameras can also be used in various ways based on research questions because cameras can be carried, placed in multiple rooms or cameras’ angle can be changed in real-time by remote control. When the required conditions are met, the video method can provide a rich collection of data. For instance, in one study, we used multiple small cameras with sufficient battery time and SD cards and hooked them on to the walls or side of the desks in the room. Remote control was utilised to start and stop the camera, and a remote control was left with the doctor so the doctor could stop the recording if the patients did not feel comfortable or the conversation topic becomes highly confidential, such as drug use or suicide.
Table 2 The benefits and drawbacks of video method and traditional observational method
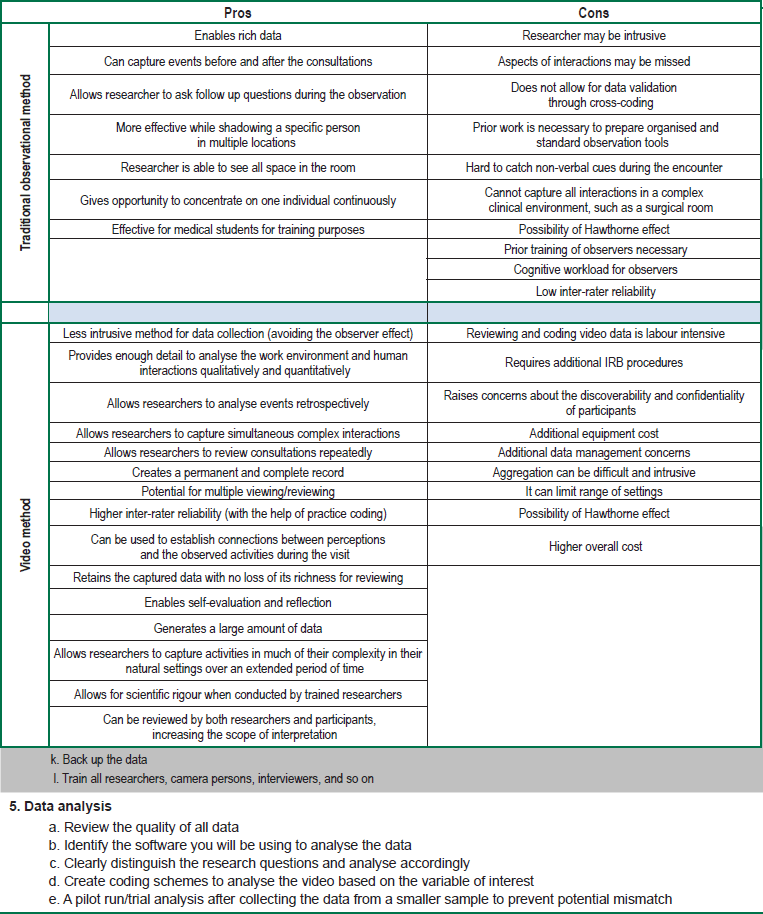
Furthermore, video method also limits the Hawthorne effect – which is the possibility of altering the behaviour of participants – since video cameras have been shown to influence participant behaviour far less than a human observer.43 However, some people may be less willing to be videotaped as opposed to live observation and feel there is more risk involved in video data due to several reasons: a) video recordings may be viewed by multiple people over time, b) outsiders may gain access to video data that are improperly stored, and c) a person’s identity may be more readily determined from a video recording than from written data. On the other hand, video data might improve ecological validity, since the video data give more complete (and visual) information about the real environment rather than traditional observers’ observation notes.
Video Data Management & Analysis
Observation data, including both video and non-video data, are confidential. However, video data introduce more risk to overall confidentiality because video data keep all interaction in a high fidelity format for several years and might be accessed by multiple people for research or non-research purposes unless sufficient precautions are taken. Video data should be stored on a secure storage without links to other identifiable information, such as address, name and social security number.32
Coding is a standard procedure to analyse the video data. Coding is an established procedure that facilitates analysing the video by identifying the tasks and interactions in the video.19 A coding scheme classifies variables of interest in the video according to the purpose of the analysis, and it speeds up the coding process. Development of coding scheme should be informed by the literature.45 Each variable in the coding scheme should be well defined, and the start and stop time of all variables should be standardised. This may help to improve the reliability of data coding and decrease biases of different coders. For example, in one study, coders were interested in the gaze direction of the doctor and patient 46 and created a coding scheme including the subject (patient or doctor) and the object of the gaze (patient, care provider, computer, chart, and so on.). This scheme allowed for a thorough and specific analysis of gaze based on subject, object and duration, such as total duration of doctor’s gaze at computer and patient during a visit.
Video data can be coded both quantitatively and qualitatively depending on the purpose of the research. Quantitative data might include the duration of specific behaviours in the visit. Software packages can help quantify all continuous behaviour (such as gazing or typing) to obtain relevant data with respective time frames.27 It is also possible to visualise the sequence of the behaviours using software. Qualitative analysis might be a thematic description of a practitioner’s behaviour during the entire visit, such as patient-focussed or computer-focussed. Qualitative data might also be gathered based on verbal communication, such as analysing turn takings and sequence of utterances.18 Some studies also used tools such as check lists (physicians’ behaviour checklist) to capture human performance data from the video recording,47 such as counting the occurrence of specific doctors’ behaviours during the doctor–patient encounter in the video data.48
Video Data and Sociotechnical Design
The components of a sociotechnical system include the individual (such as health care workers), tasks, tools and technologies, the physical environment and organisational conditions.69 It is essential to understand users of the system and interactions among these users in real settings to address sociotechnical design concerns.70 It is also necessary to better understand the impact of boundaries on sociotechnical systems and their implications for physical, cognitive and psychosocial ergonomics. Furthermore, effective design, implementation and use of newly introduced technologies into the overall system is strongly related to the fundamentals of human factors ergonomics.71 A number of studies have focussed on the concept of sociotechnical factors that complicate health information systems deployment,72 including the interaction between the technical features of a health information system and the social features of a health care work environment.73 After a new system implementation, sociotechnical interactions have a direct effect on the success of the process. In the future, many new medical technologies will be introduced into the system. Video recording might also be a strong tool to explore technology interventions, which can make sociotechnical systems more effective and efficient. For instance, video data can be used to analyse the current medical technology, such as electronic health records (EHR) and to inform how new EHR can be integrated into the sociotechnical system more effectively.
